(0933) Expanding Tympanoplasty: Utilization of Anterior External Auditory Canal Drilling and Vascular Strip in Transcanal Approaches
Monday, September 30, 2024
12:00 PM - 1:00 PM EDT
Disclosure(s):
Shannon Robins: No relevant relationships to disclose.
James E. Saunders, MD: No relevant relationships to disclose.
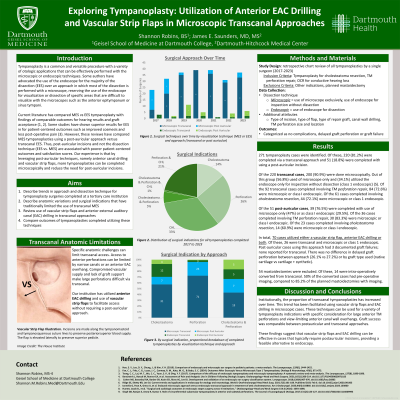
Introduction: Transcanal tympanoplasty is limited primarily by the size and location of perforations. Additional anatomic features such as narrow ear canals or anterior canal bulges that limit visualization further restrict traditional transcanal approaches. This study describes the utilization of anterior EAC canal wall drilling and vascular strips in the setting of transcanal tympanoplasty and evaluates the graft outcomes of these techniques.
Methods: A retrospective chart review was performed for patients undergoing a transcanal tympanoplasty for perforations, cholesteatomas or conductive hearing loss (CHL) by one surgeon from 2019-2023. Surgeries involving anterior EAC drilling and/or vascular strips were identified. Additional surgery attributes included size and location of perforation, graft type, and the use of native or prosthetic ossicle reconstruction. The primary outcome measure was postoperative graft complications such as recurrent perforation and revision surgery.
Results: Of the 195 transcanal tympanoplasty surgeries, 23 (12%) involved drilling the anterior EAC wall, mobilizing a vascular strip, or both. Native cartilage grafts were utilized for 11 of these cases, while native cartilage grafts with synthetic submucosa grafts were used for 12 cases. Of the transcanal surgeries with these techniques, 6 (26%) had postoperative graft complications; all complications described were recurrent perforations. A single surgery required revision. There was no difference in complication rate between cases that used only native cartilage grafts (27%) versus native plus synthetic grafts (25%) in this cohort.
Conclusions: Data from this chart review describes the feasibility of using anterior EAC wall drilling and/or vascular strips in transcanal tympanoplasties typically limited by their anatomical restrictions or defect location. Use of these techniques had no appreciable difference in outcomes. EAC drilling and vascular strips should be considered for transcanal tympanoplasty, especially in the setting of moderately large anterior perforations or unfavorable bony canal anatomy.